Knee
Knee Anatomy :: Knee Arthroscopy :: ACL Reconstruction :: Total Knee Replacement
Uniknee Replacement :: Revision Knee Replacement :: Multiligament Knee Reconstruction
Knee Osteotomy :: Patellar (Knee Cap) :: Knee Fracture & Lower Limb Fracture
Posterior Cruciate Ligament (PCL) :: Chondrocyte Grafting
Normal Anatomy of the Knee Joint
How does the Knee joint work?
Find out more in this web based movie.
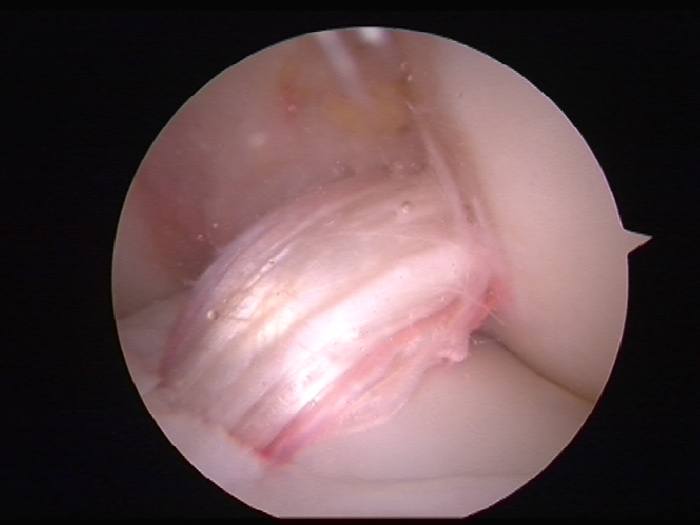
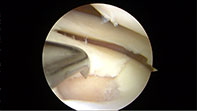
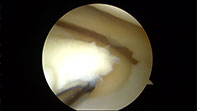
Knee Arthroscopy
Arthroscopy is a surgical procedure in which an arthroscope (camera) is inserted into a joint. The benefits of arthroscopy involve smaller incisions, faster healing, a more rapid recovery, and less scarring. Arthroscopic surgical procedures are often performed on an outpatient basis and the patient is able to return home on the same day.
Conditions treated by Arthroscopy
- Meniscus Tear
- ACL/PCL injury
- Synovitis
- Chondral flap
- OCD lesion
- Knee cap release
- Loose bodies
Patient Presentation
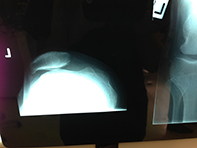
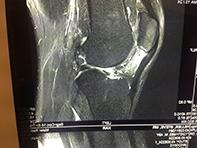
Patients usually present following an acute injury to their knee. Pain is the most common presenting symptom. Some patients may experience clicking, catching, locking, giving way or knee swelling. As part of the diagnosis and work up, patients often require a plain xray and MRI scan.
Surgical Risks
Knee arthroscopy is generally regarded as a safe procedure with minimal patient risk. Some of the rare risks associated with this procedure include:
- Bleeding into the joint (haemarthrosis) - 1 in 100
- Infection - 1 in 1000
- Damage to the cartilage or meniscus
- Failure of the surgery to relieve symptoms
- Knee stiffness
- Scaring of the skin or lump under the wound
- Deep Vein Thrombosis (DVT) - 1 in 750
- Pulmonary embolus (PE) - risk 1 in 3000
- Severe pain (Complex Regional Pain Syndrome) - rare
Post Operative
Following surgery you will go to the recovery room for a short period and then back to the Day Admissions ward. You will be allowed home once you have eaten something and also have mobilized safely. Occasionally some patients require crutches. You will have small waterproof dressings on the wounds with a large dressing which can be removed the day following surgery. You will also have an ice pack and we encourage regular icing over the first week. Patients are discharged with a prescription for pain killers and may also need anti-inflammatories. All patients will be reviewed by your surgeon prior to discharge and will be seen again in rooms 10-14 days post surgery.
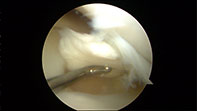
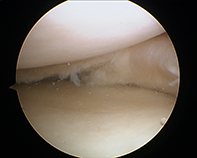
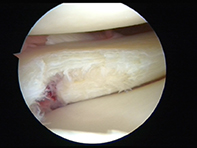
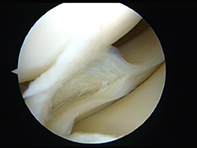
Click on the thumbnails for enlarged view
-
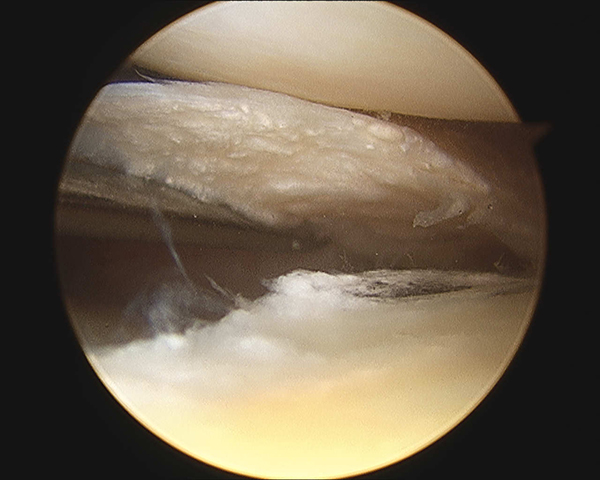
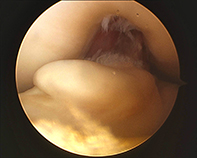
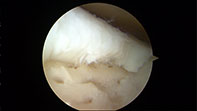
Bucket Lateral Meniscus

-
Bucket Handle Tear Meniscus
-
Bucket Handle Tear Medial Meniscus

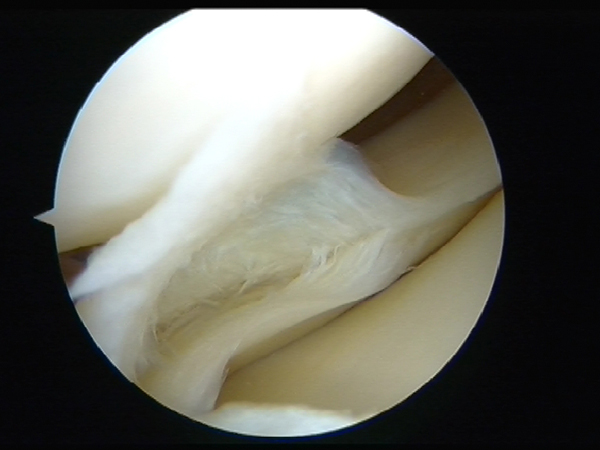
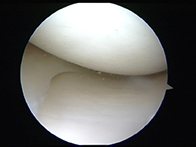
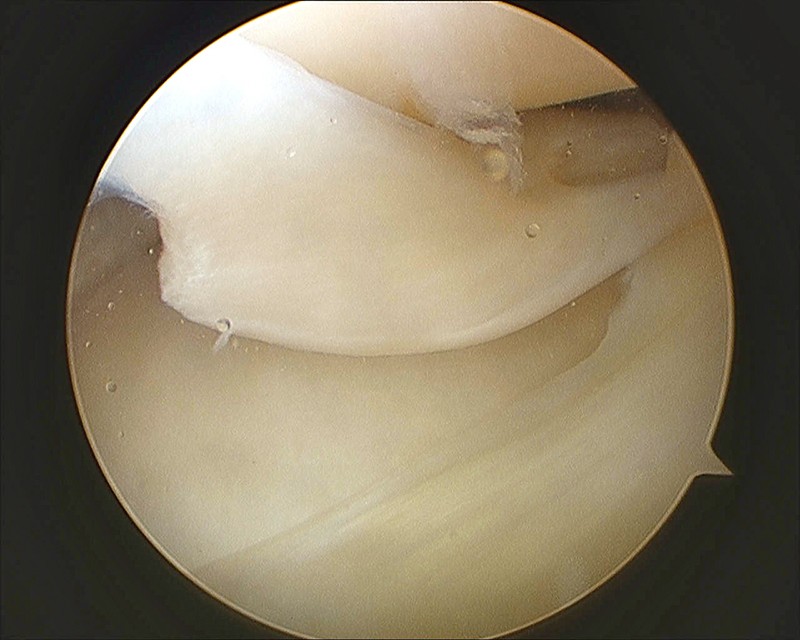
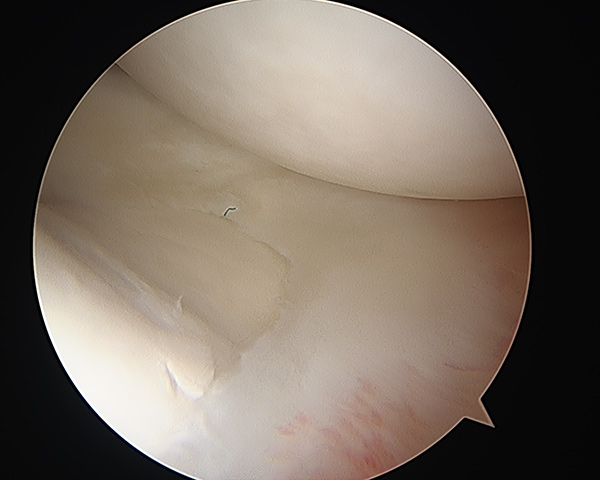
Normal Knee Cartilage And Medial Meniscus
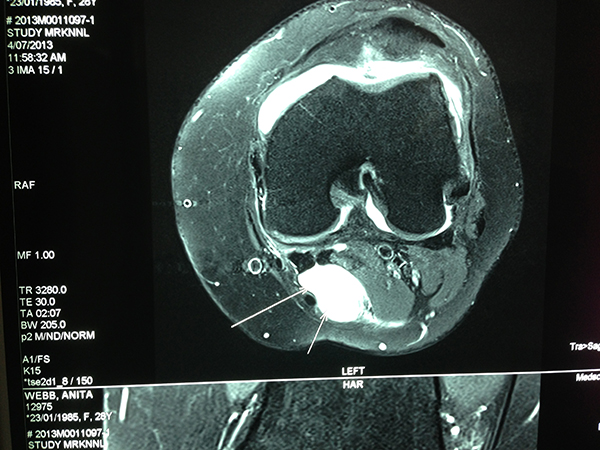
MRI Of Lateral Parameniscal Cyst

-
Loose

-
Loose Body
-
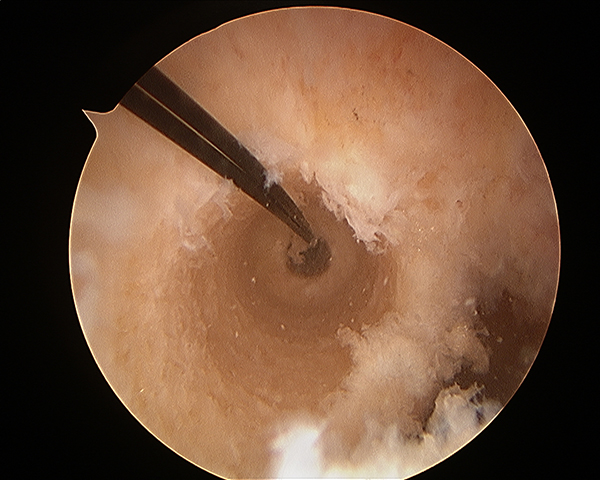
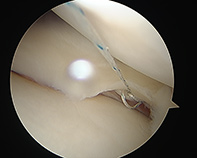
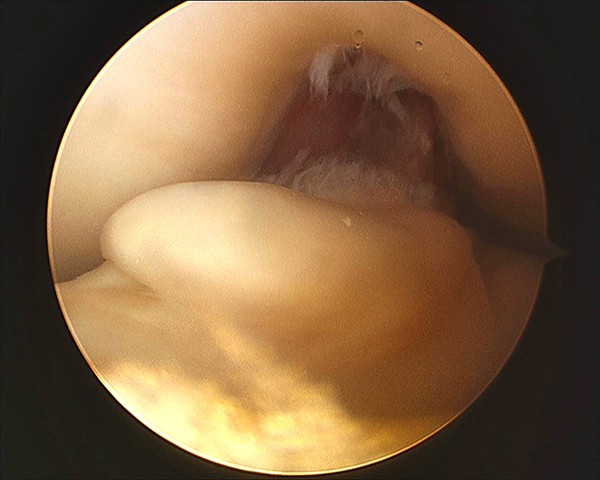
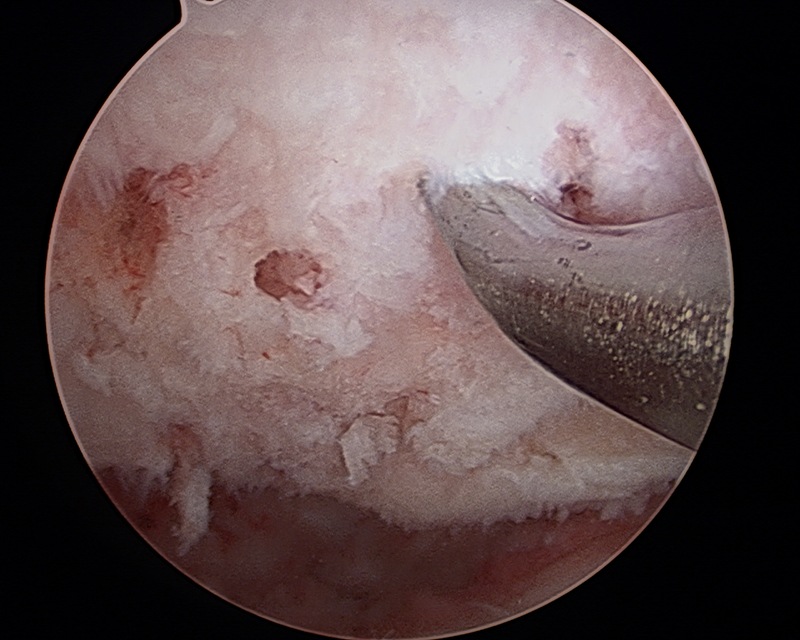
Microfracture
-
Microfracture IFC
Bakers Cyst
Cyclops Lesion
Ganglion From TIB FIB

-
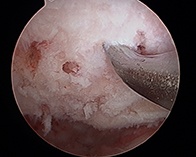
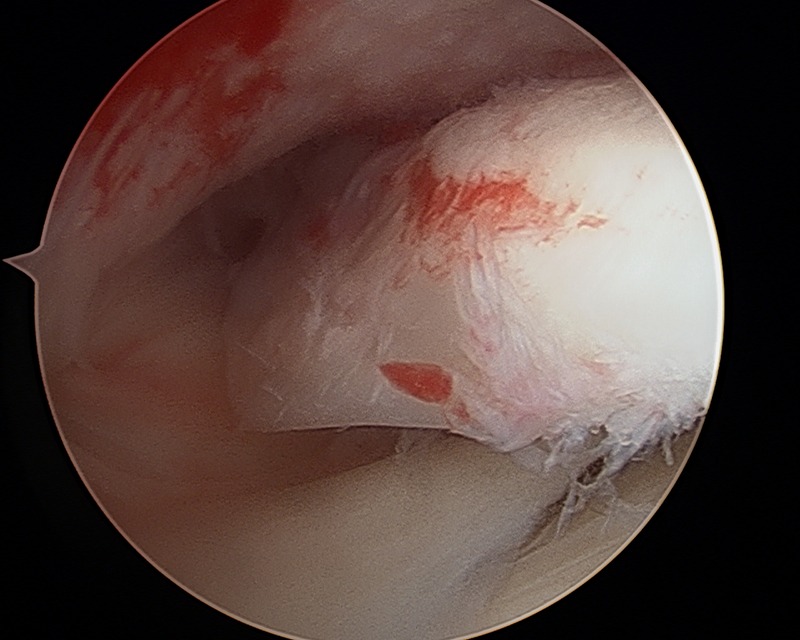
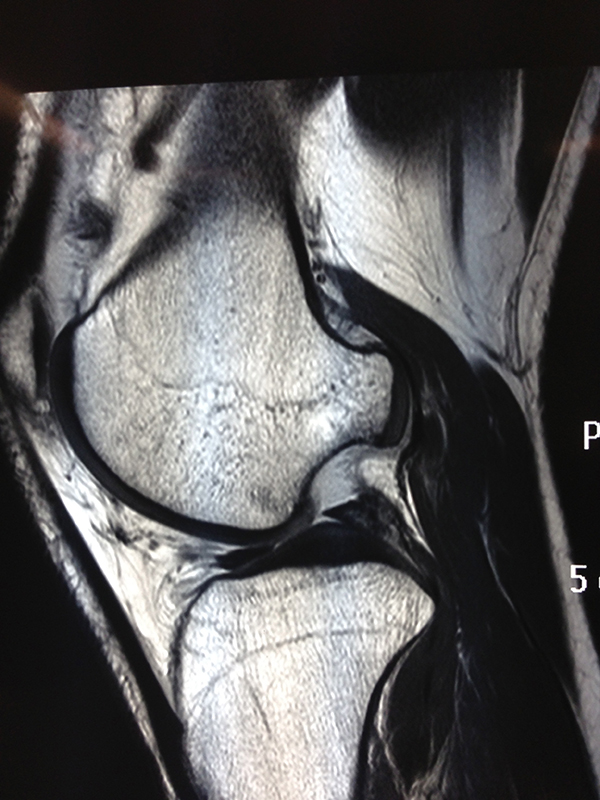
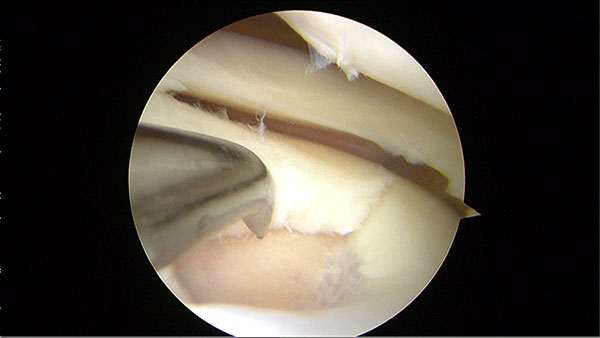
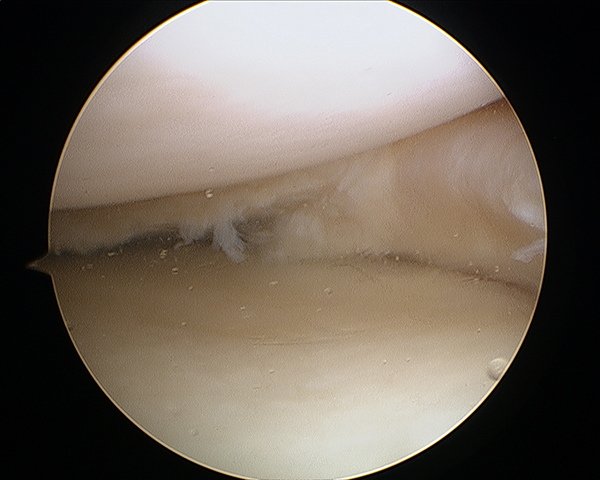
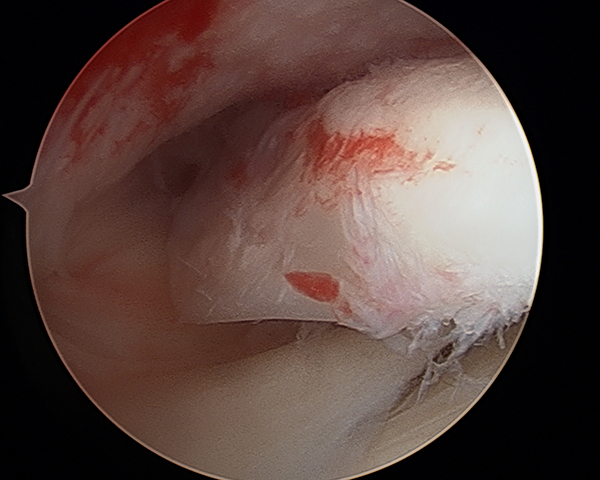
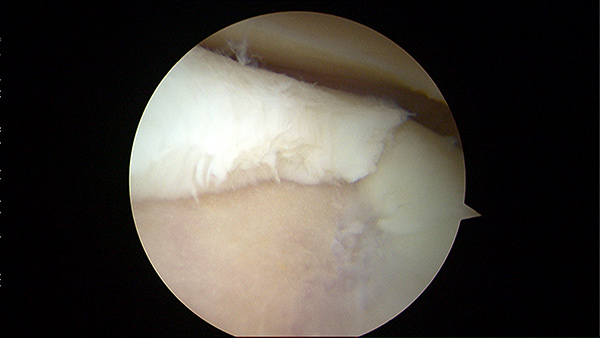
Chondral Defect

-
Chondral Fragment
-
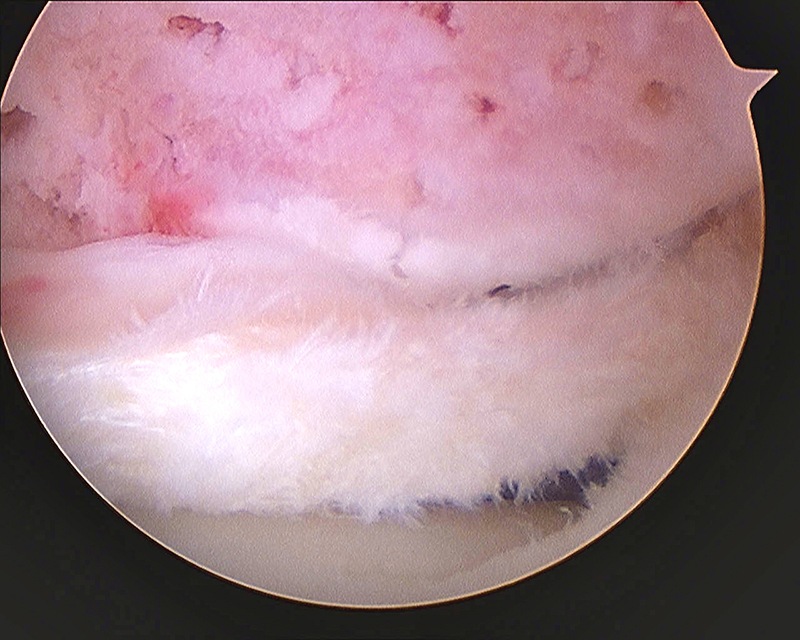
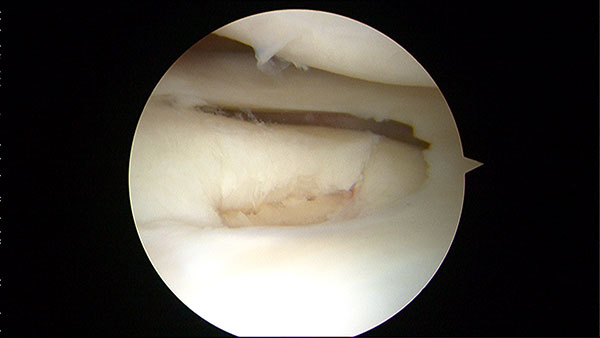
Chondral Defect
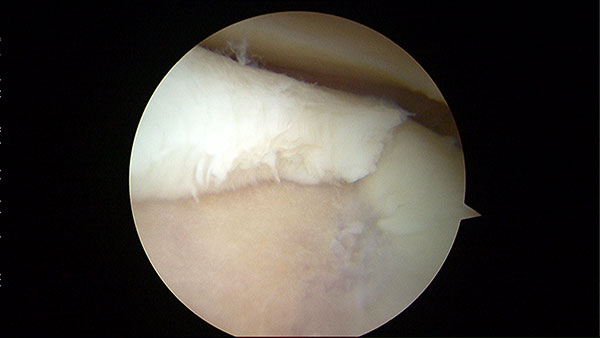
Chondral Tibial Flap And Microfracture
Chondral Tibial Flap And Microfracture

-
Chondral Tibial Flap And Microfracture

Discoid Lateral Meniscus

-
Discoid Lateral Meniscus
-
Discoid Lateral Meniscus
-
Chondral Tibial Flap And Microfracture
-
Chondral Tibial Flap And Microfracture
-
Chondral Tibial Flap And Microfracture
-
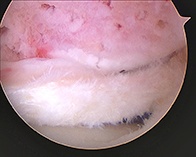
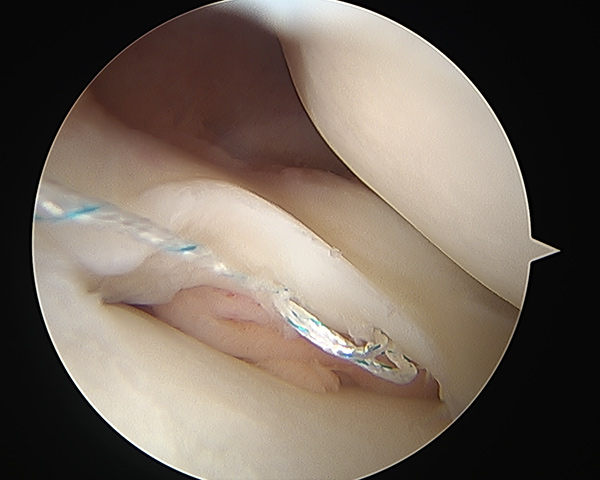
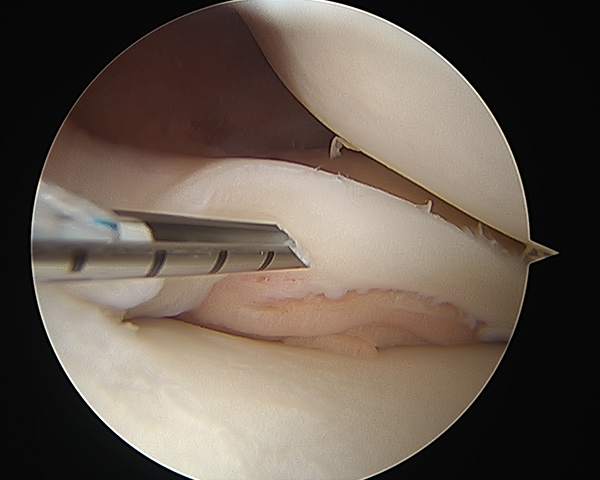
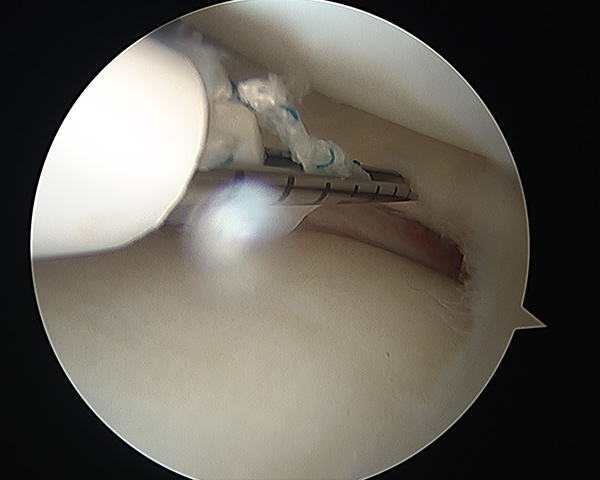
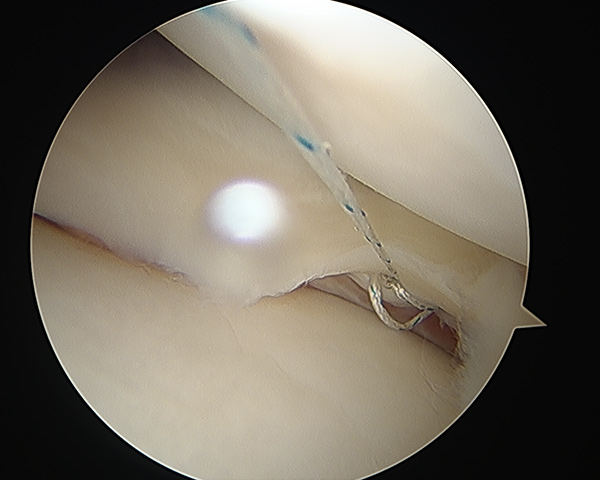
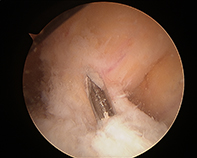
Lateral Meniscus Repair

-
Lateral Meniscus Repair
-
Lateral Meniscus Repair
Lateral Meniscus Repair
-
Lateral Meniscus Repair

-
Loose Body
-
Bicondylar TIB Plateau Fracture

-
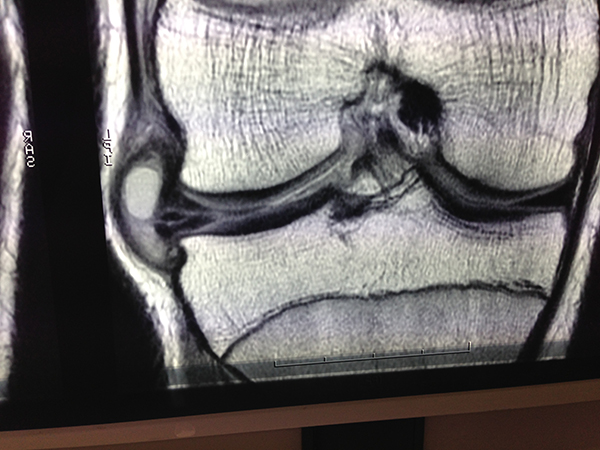
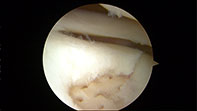
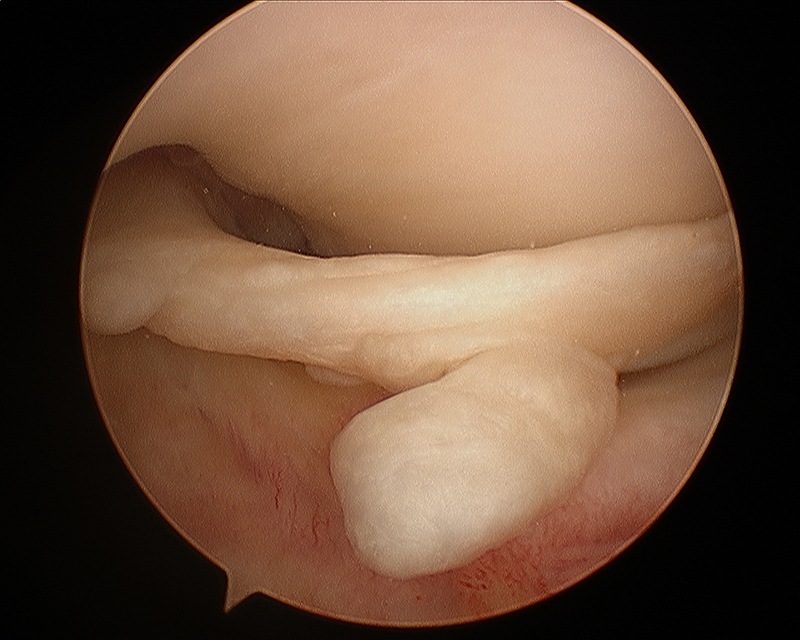
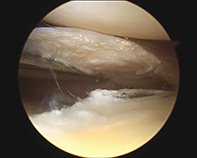
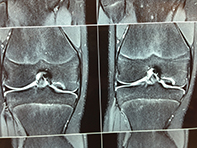
Double Bundle Bucket Handle Medial Meniscus
-
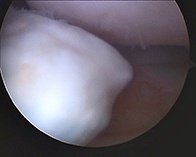
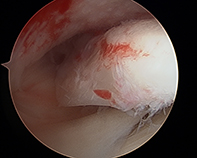
Large Loose Chondral Fragment
-
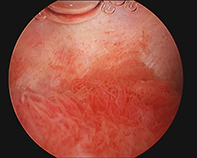
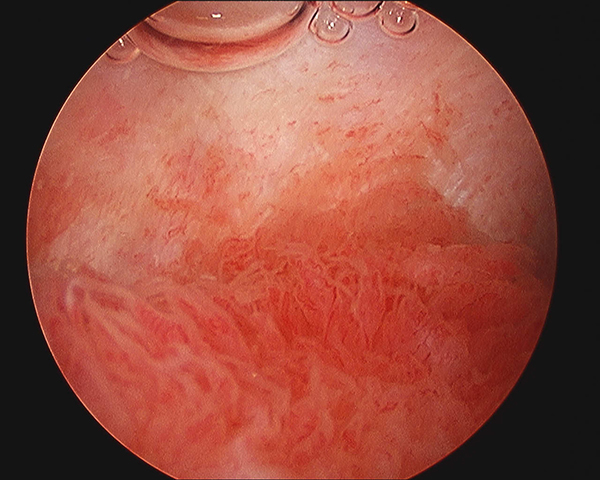
Severe Synovitis
-
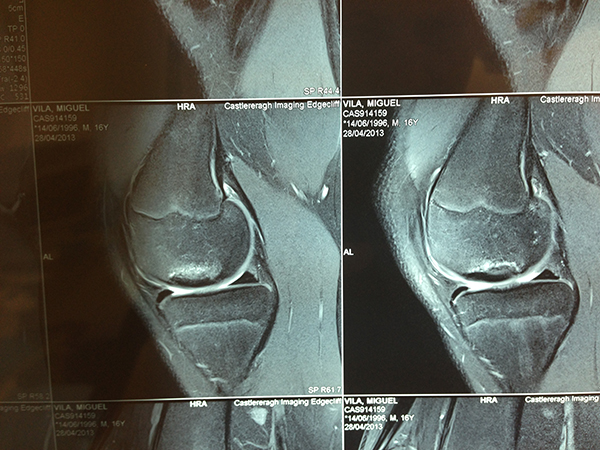
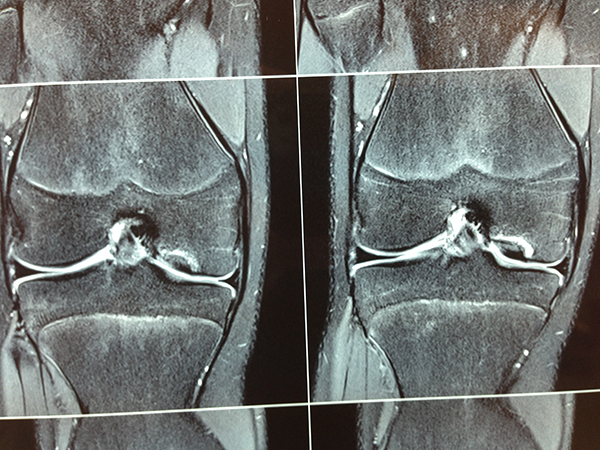
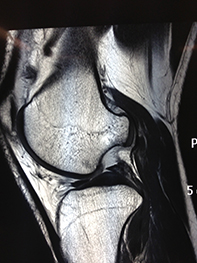
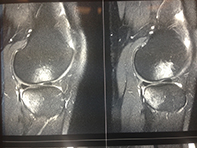
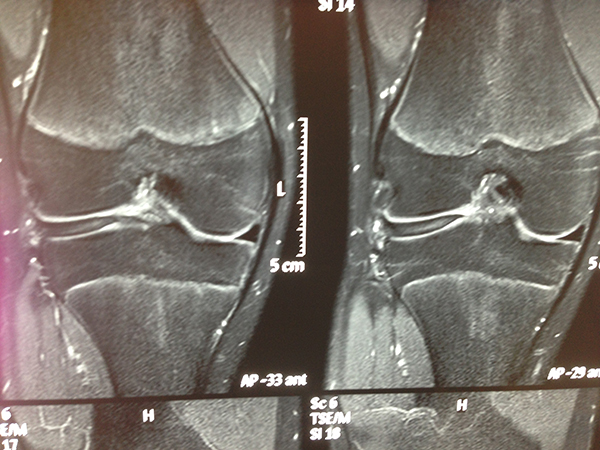
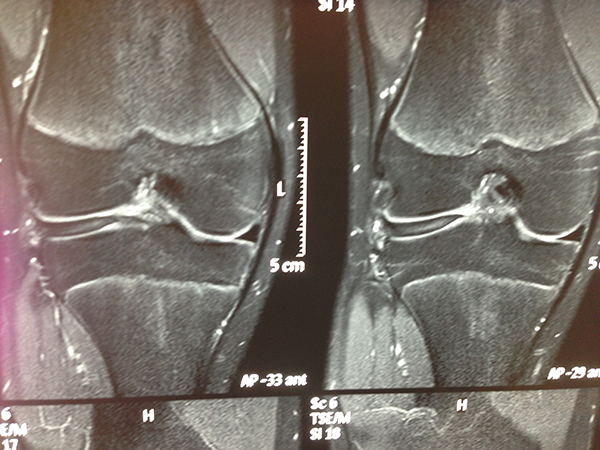
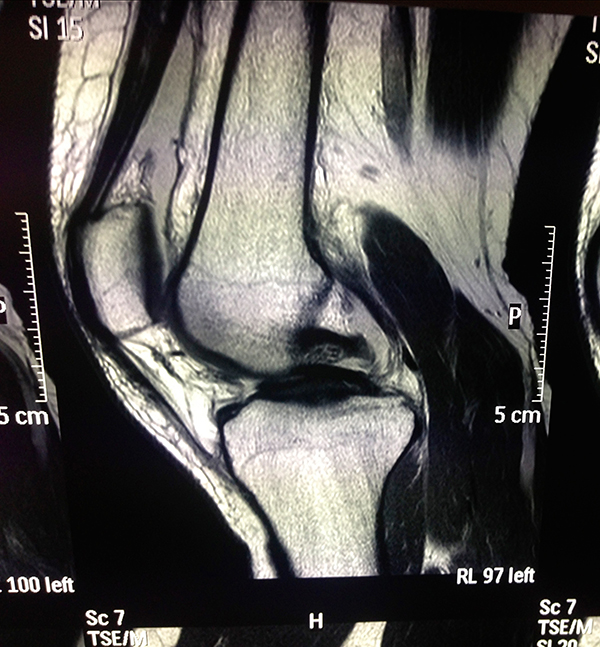
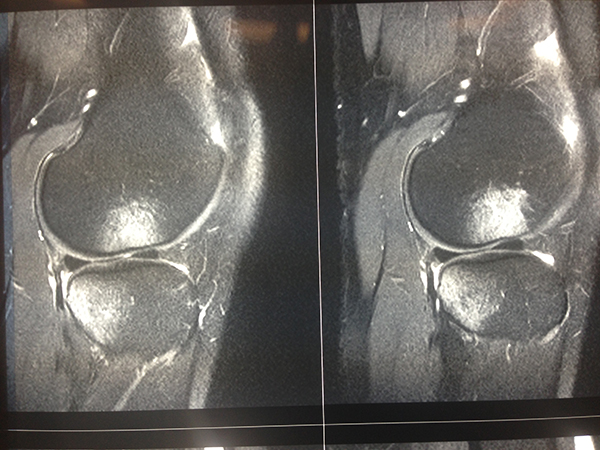
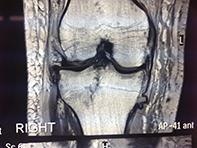
Bony Bruising Pattern ACL Tear
-
Loose OCD
-
Chondral Tibial Flap And Microfracture
-
Chondral Tibial Flap And Microfracture
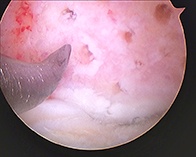
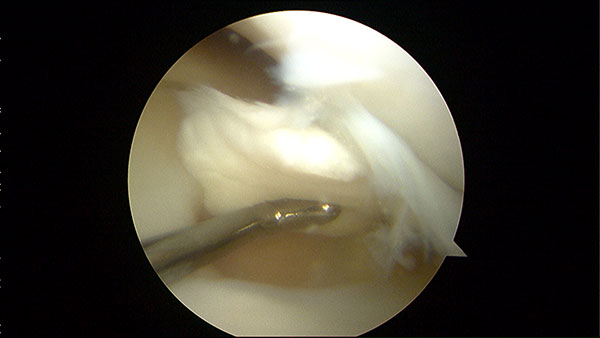
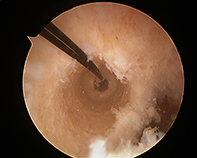
Performing Microfracture













Positive Lachmann
Anterior Cruciate Ligament Reconstruction
The anterior cruciate ligament is one of the major stabilizing ligaments in the knee. It is a strong rope like structure located in the centre of the knee running from the femur to the tibia. When this ligament tears unfortunately it doesn't heal and often leads to the feeling of instability in the knee.
ACL reconstruction is a commonly performed surgical procedure and with recent advances in arthroscopic surgery can now be performed with minimal incisions and low complication rates.
History and Examination
Patients often give a classic history of their injury. It usually occurs following a non contact pivot injury to the knee however can also occur during contact sports. Classic features of the history include:
- Twisting knee injury
- Heard a pop
- Felt a clunk
- Could not play on
- Knee swelling within 4 hours if injury
- Severe Pain
- Knee gives way
As part of the work up, patients require a plain xray and MRI of the knee.
Do I need an ACL reconstruction?
The ACL does not tend to heal itself. It is within the knee joint and the joint fluid prevents healing. A new ligament must be reconstructed using another tendon. If you play pivoting sports or have symptoms of instability in daily life consider ACL reconstruction. I would recommend surgery in most patients who wish to continue participation in sport or physical work.
There are definite benefits to surgery. It provides knee stabilization and prevents further damage to structures inside the knee particularly the meniscus and cartilage surfaces of the femur and tibia.
Timing of Surgery
Timing of surgery varies between patients. It is generally recommended that patients have surgery within 6-8 weeks post injury. You must have regained a full range of motion of the knee joint and most of the swelling must be resolved prior to surgery. Some patients have an injury to the medial collateral ligament (MCL) as well as the ACL tear and require a period of knee bracing pre-operatively to allow the MCL to heal. I do not perform the surgery until stiffness is fully resolved.
Graft Types
Many graft types are available to use. These include:
- Hamstring tendons
- Patella Tendon
- Quads tendon
- Allograft
- Artificial graft (LARS)
Most surgeons in Australia perform a 4-strand hamstring graft which is stronger than the native ACL. I prefer to use a 5-strand hamstring graft which allows for larger bone tunnels for the graft and indeed a stronger graft. I also regularly use a middle third patellar tendon graft. The long term results and survival of both these grafts in the literature are similar.
The LARS ligament has received a lot of media publicity following its use in some high profile athletes. Only short-term outcomes were available. There are surprisingly few studies reporting on LARS ligament outcomes. Only short term outcomes are available. We do know that shedding of synthetic debris from this ligament inside the knee can cause synovitis and predispose to early arthritis. It is my preference to not use the LARS ligament for primary ACL reconstruction.
Specific Risks of surgery: are all relatively small
- Infection
- Deep Vein Thrombosis
- Excessive bruising and swelling
- Joint stiffness
- Graft Failure 5-10%
- Numbness
- Nerve or vessel damage
- Donor site problems
- Hardware Problems
- Residual Pain and swelling
Recovery
Following surgery the patient will remain in hospital for one night and will have three doses of post operative antibiotics. The majority of patients will not require a brace and will be bearing full weight as tolerated with crutches upon discharge. I advise early involvement with physiotherapy to for swelling control and knee range of motion. As a rough guideline, patients will be on crutches for 2 weeks, jogging in a straight line by 3 months and running with pivoting by 7 months. A return to competitive or contact sport will be 9-12 months.
Physiotherapy is an extremely important part of recovery. The time commitment to this part of the overall treatment is approximately 9-12 months however your physiotherapist will be your guide.
Rooms Pivot Shift
Rooms Lachmann
MCL
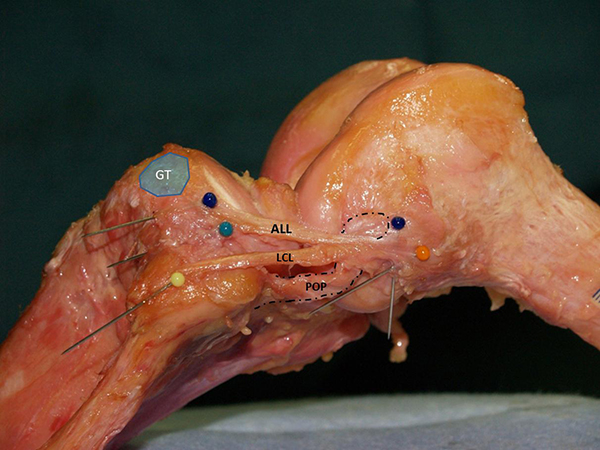
Deficient ACL, Anterolateral Instability
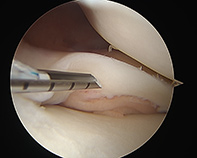
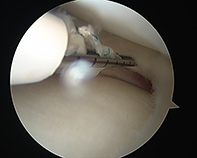
Click on the thumbnails for enlarged view
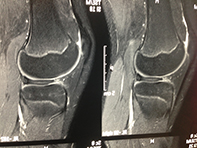
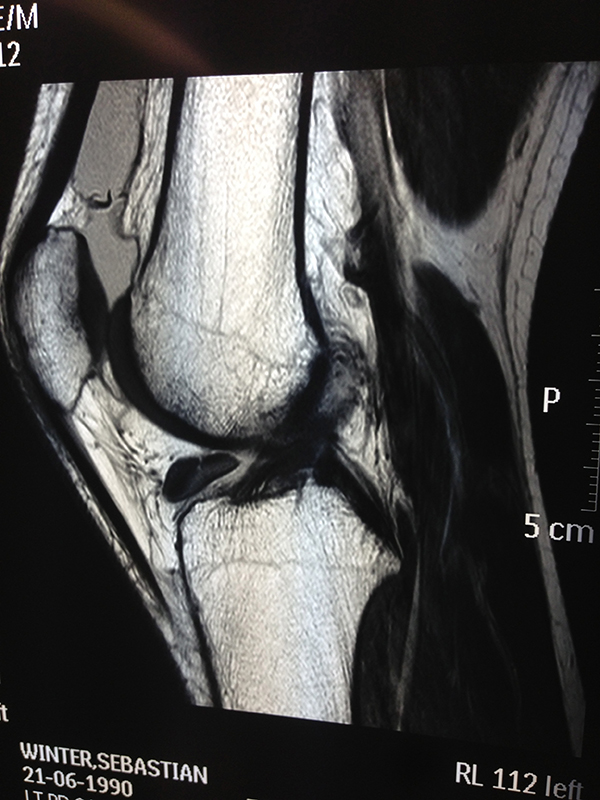
Bone Bruising With Patella Dislocation

-
Patella Dislocation

Bucket Handle Tear Medial Meniscus
-
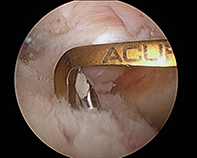
ACL Femoral Tunnel Drill
-
ACL Tibial JIG
-
ACL Tunnels Passing Graft

-
ALL

-
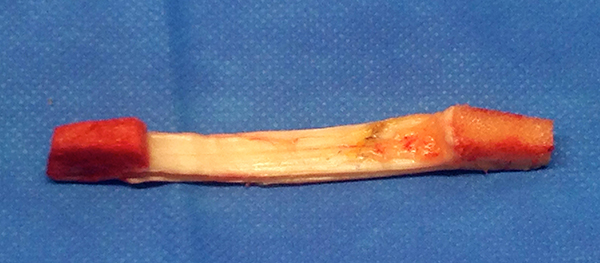
Bone Pattellar Tendon Bone Graft

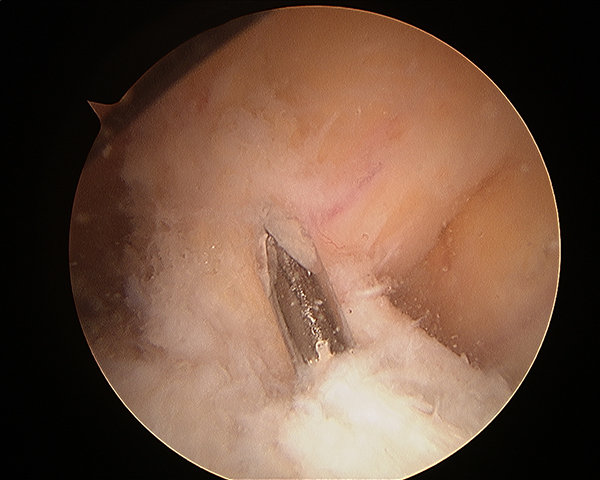
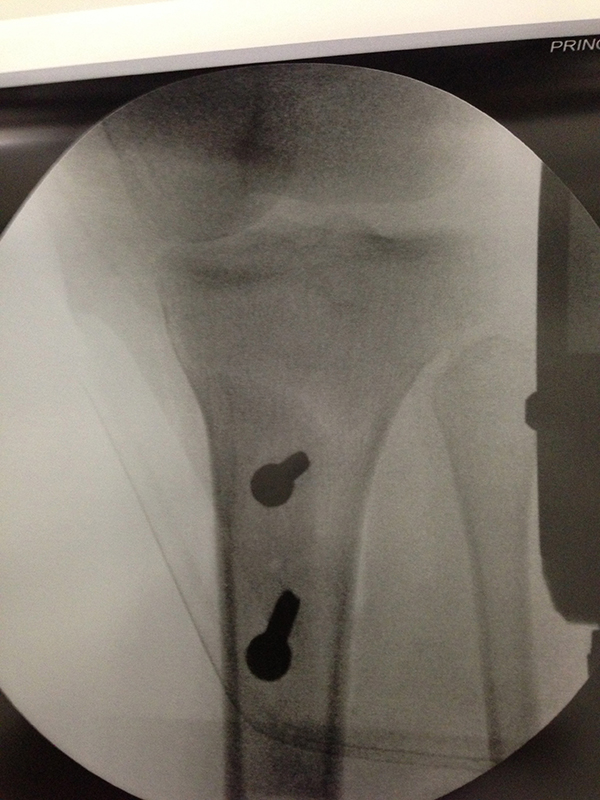
ACL Wire Tibial Foot Print
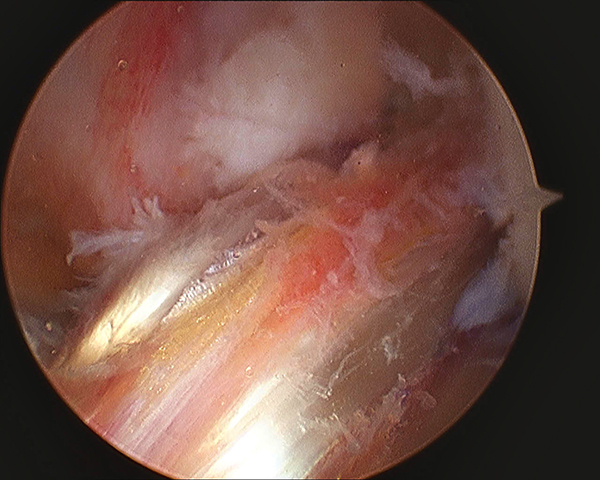
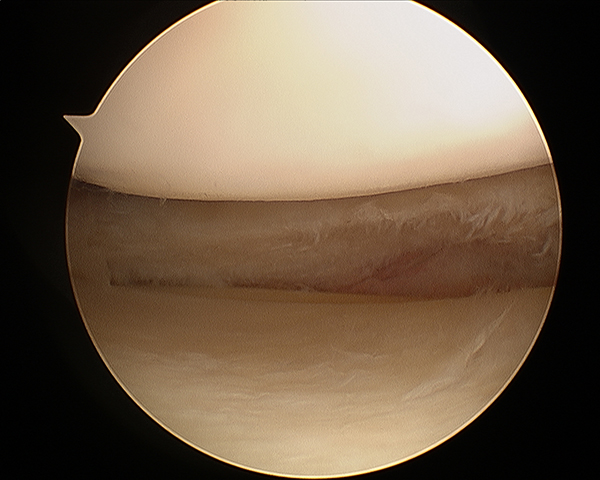
New ACL Graft

Chondrocalcinosis
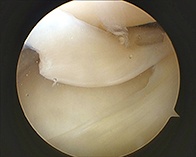
Post Meniscal Debridement
Patellar (Knee Cap) Problems & Instability
Overview
Knee cap (patellofemoral) instability occurs when the knee cap does not slide centrally within the grove of the thigh bone (Trochlea). The knee cap can partially come out of the groove (subluxation) or completely come out of the groove (dislocation).
Our assessment of patients with patellofemoral instability has improved recently as our knowledge of patello-femoral joint anatomy and its stabilizing factors has increased.
Accurate assessment of the underlying abnormailities in the unstable joint enables formulation of appropriate management plans.
Patellar pain is common in both athletic and nonathletic individuals. Among athletes, men tend to present with more patellofemoral injuries, including traumatic dislocations, than women. In the nonathletic population, women present more commonly with patellar disorders. The three most common causes for patellar dislocation remain: traumatic dislocation, trochlear dysplasia (flattening) and maltracking secondary to bone malalignment. It is essential to understand the underlying cause in order to direct appropriate treatment.
Patellofemoral problems are mainly diagnosed by obtaining a thorough history and performing a physical examination. Imaging studies help confirm the diagnosis. Plain radiography is not as sensitive as magnetic resonance imaging (MRI), but it is the least expensive and most readily available modality.
In general, surgery is more effective in preventing recurrences of dislocation because skeletal and muscular components of the patellofemoral joint and extensor mechanism are realigned; however, surgery also has risks. In a patient with normal anatomy, surgery should be considered an option after all conservative treatment modalities are unsuccessful. Patients with anatomic abnormalities may benefit from earlier surgical consideration.
Clinical History
Facts about recurrent instability include
- Female teenagers are the most common first time dislocators
- After a first time dislocation there approximately 17% will have further problems
- If previous subluxation or dislocation, 50% will have further episodes of instability
- The younger the age at first dislocation, the higher the risk of subsequent dislocation
- More severe initial dislocation = higher risk of recurrent dislocation
- Further risk factors are a family history of patella instability and the risk factors for developmental dysplasia of the hip (first born girl, high birth weight, breech delivery, Caesarian)
Imaging of the Knee with Chronic Instability
These are the imaging techniques and measurements I use for reliability and simplicity and the benefit they provide in decision making.
- X-rays These can show, Patella alta, Trochlea dysplasia
- CT scans – CT scans have been widely used in the assessment of chronic instability. I mainly use CT scan to assess complex rotational alignment deformity
- Magnetic Resonance Imaging (MRI) – MRI scans will reliably demonstrate
Bone abnormalities – Trochlea and patella dysplasia
Large cartilage injuries to the patellofemoral region
Patella tilt any abnormalities to the static constraints e.g. medial patellofemoral ligament rupture and patella alta
Bone bruising of a recent dislocation will be seen on these images
Although far more expensive, MRI is more effective than CT scanning in determining if patellar chondral lesions are present and for determining cartilage thickness and volume. Assessment of patellar cartilage thickness and volume is important to evaluate for osteoarthritis.
Axial views on MRI or CT scans may be used to evaluate the trochlea-tubercle (TTTG) distance. This is the horizontal distance in a vertical plane between the intercondylar notch and the tibial tubercle. Similar to the Q-angle, this evaluates the potential laterally directed vectors on the patella. Some authors suggest that a distance of 2 cm is specific, but not sensitive, for maltracking.
Physiotherapy
During the acute phase of a patellar injury or dislocation, the immediate goals are to reduce inflammation, relieve pain, and stop activities that place excessive loads on the patellofemoral joint. Physiotherapy is an essential component of treatment.
Quadriceps strengthening is initiated during the acute phase. In the event of acute patella dislocation, these should be static exercises initiated during the period of immobilization. Reduction of swelling and regaining knee range of motion are also primary goals. Therapy should also include a protocol for hamstring muscle stretching. Tight hamstring muscles functionally counteract their agonist group, the quadriceps.
Patellar taping (McConnell method)
- The goals of McConnell taping are to restore proper alignment and control pain
With proper alignment, VMO (quadriceps muscle) retraining is initiated. Once taped, patients should note decreased pain when performing painful activities. The goal of taping is to optimize patellar positioning and facilitate better activation of the medial (inner) patellar stabilizers, particularly the VMO. The technique can be taught to patients to perform themselves. This method was described by a Sydney based physiotherapist and is now used in practice worldwide.
Formulating a Surgical Management Plan
Surgery is only considered if non-operative treatment has failed and the recurrent nature of the disease has resulted in functional impairment.
Surgery may be directed toward either bone or soft tissue components.
I believe the surgical strategy should, wherever possible, aim to restore normal anatomy to the joint, rather than introduce new abnormalities. I will discuss what I believe will be the best option for you.
Bone Procedures
- Rotational Oteotomy – Breaking the bone and fixing it in a new position to get the knee cap to track better
- Tibial Tubercle Osteotomy – Moving the bony attachment of the patella
- Soft Tissue procedure
- Medial patellofemoral ligament reconstruction – Using the hamstrings tendon to reconstruct the MPFL
- Lateral release – Releasing tight tissues on the outside of the patella
- Medial imbrication – Moving the muscle acting on the patella
Presence of Arthritic Change in the Patellofemoral Jointstrong>
In the presence of degenerative joint disease (cartilage damage), surgical treatment becomes difficult with a guarded outcome. If the articular lesion is localized to only one side of the joint then cartilage healing (micro fracture) or cartilage restorative (eg MACI or OATS) procedures can be used.
If degeneration is present on both joint surfaces, salvage surgery will be required.
Options include chondroplasty(shaving loose cartilage), lateral release (releasing tight tissue on the side of the knee cap) and tibial tubercle elevation (reseting the position of where the patella tendon attaches).
With failed surgery or advanced arthritis (wear and tear), partial knee replacement or total knee replacement are the only options.
Dislocating Patella
J Tracking Patella
-
Ganglion Tib Fib

-
Horizintal Cleavage Tear Meniscus
-
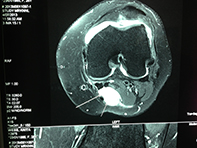
Trochlea Dysplasia
-
Axial Mri Patella Dislocation

-
MRI Lateral Parameniscal Cyst

-
Patellar Tendinopathy
-
Osteochondral Defect MFC

Osteochondral Defect MFC
-
Patellar Tendinopathy
-
Tibial Tubercle Osteotomy

-
Tibial Tubercle Osteotomy

Dr. Solomon's Knee Arthritis information:
There are many misleading statements in the media , on the internet as well as claims made by providers who claim that certain tablets, injections or even stem cells can reverse the arthritis process. Unfortunately most of these claims are completely false. There is NO scientific literature evidence that proves that by taking a certain tablet or having an injection into your knee, you arthritis will resolve. There is nothing that can stop a knee joint that has started to wear out from continuing to wear out. There are measures however that can assist with pain management before surgery is indicated.
Stem Cells:
Is this stem cells or stem “sells “ !
We all would like to believe that stem cells would cure our arthritis. Unfortunately this is not the case and NO controlled scientific study has shown this. There are ongoing studies looking at how an injection of stem cells may affect the knee. We are still awaiting the outcome of studies that prove one way or another that stem cells will be a useful addition to the treatment of knee arthritis. Stem cell injections cost close to $9000 and personally I would not be spending that type of money when there is no proof that it will fix my knee pain and reverse my arthritis.
I am all for ongoing research into this area however I would caution patients when deciding whether to spend a fortune on something that is still experimental.
Knee Replacement Surgery
Similar to hip replacement surgery, a knee replacement is indicated when you have advanced osteoarthritis of the knee joint and non-operative measures (eg. Weight loss, anti-inflamatories , physiotherapy etc) are no longer controlling your pain.
Modern day knee replacements are a successful way to treat end stage arthritic knee pain and immobility. It is never really too late to replace the knee so if you can manage with your current arthritic knee……………. keep going until such time as it becomes too uncomfortable and is interfering with your quality of life.
Types of Replacement:
Arthritic knees that require surgery usually require a Total Knee Replacement. A unicompartmental or “half knee” replacement is reserved for a select few patients who have knee arthritis isolated to one area of the knee joint and who satisfy other preoperative criteria. The revision rate of a unicompartmental knee replacement is significantly higher that a total knee replacement (16% vs 6% at 11 yrs) and therefore there are strict requirements in patient selection.
The 2012 Australian National Joint Registry shows that successful knee replacements have an average of 6% revision rate at 11 years following surgery and that if you are over the age of 65 your revision rate is less than 5% and over the age of 75 your revision rate is less than 3%. Younger patients have higher rates of revision.
A total knee replacement is designed to resurface the femur, tibia and patella and in-between the femur and tibia is a layer of polyethelene. The polyethelene (plastic shock absorber) is the bearing surface which ALL knee replacements use. Unlike in hip replacement surgery there is no ceramic on ceramic knee replacement bearing. There is also NO metal on metal bearing so the problem that happened with some metal on metal hip replacements does not exist in knee replacements.
It is anticipated (laboratory studies) that a well aligned and functioning knee replacement should last around 25-30 years before the plastic wears out.
You may have heard about computer navigation , patient specific instruments etc. These are simply tools that some surgeons use to align the replacement during surgery. There are no scientific studies that have proven that a standard surgical technique using instrumentation is any better than computer navigation or patient matched blocks PROVIDED the surgeon doing the surgery is a competent surgeon who aligns the implants correctly and balances the knee joint appropriately.
In other words choose a surgeon who is skilled at would he does using ANY method and you should have a good long term outcome.
Cement or no cement:
Knee replacements may either be cemented onto the bone or used in an uncemented fashion where the bone grows onto the prosthesis. There is no scientific evidence that one method is better than the other. My preference has always been to use cement, as patients tend to recover a little quicker in terms of pain and comfort.
The final word on knee replacement.
Surgery is indicated when non-operative measures no longer control the pain and your quality of life is significantly affected. Over 85% of knee replacements will achieve a good pain free functional result however there are some patients (around 5%) that may still have a niggling ache in the replaced knee joint.
Patients are able to play sport including golf, ski, tennis, bowls, cycle, swimming etc HOWEVER a knee replacement is not designed for impact sports such as running, contact sports, basketball, squash and any sport that results in constant and significant impact on the knee.
We tend to ignore our knees until something happens to them that causes pain. If we take good care of our knees now, before there is a problem, we can really help ourselves. In addition, if some problems with the knees develop, an exercise program can be extremely beneficial. To understand the functions, conditions, surgeries & procedures of the knee better, we have included an interactive animated presentation.
Total Knee Replacement (TKR)
A total knee replacement (TKR) or total knee arthroplasty is a surgery that resurfaces an arthritic knee joint with an artificial metal or plastic replacement parts called the ‘prostheses'.
Find out more about Total Knee Replacement with the following links.
Anterior Cruciate Ligament ACL Reconstruction
The anterior cruciate ligament is one of the major stabilizing ligaments in the knee. It is a strong rope like structure located in the centre of the knee running from the femur to the tibia. When this ligament tears unfortunately it doesn't heal and often leads to the feeling of instability in the knee.
ACL reconstruction is a commonly performed surgical procedure and with recent advances in arthroscopic surgery can now be performed with minimal incisions and low complication rates.
ACL Reconstruction Hamstring Tendon
ACL Reconstruction Patellar Tendon
Unicompartmental Knee Replacement
Partial knee replacement or Uni knee replacement is a treatment option that replaces (or resurfaces) only the damaged portion of the knee while conserving knee ligaments and unaffected cartilage.
Find out more about Unicompartmental Knee Replacement with the following links.
Revision Knee Replacement
This means that part or all of your previous knee replacement needs to be revised. This operation varies from very minor adjustments to massive operations replacing significant amounts of bone and hence is difficult to describe in full.
Find out more about Revision Knee Replacement with the following links.
Multiligament Knee Reconstruction
Coming soon
Find out more about Multiligament Knee Reconstruction with the following link.
Knee Osteotomy
Coming soon
Find out more about Knee Osteotomy with the following link.
Knee Fracture & Lower Limb Fracture
Coming soon
Find out more about Knee Fracture & Lower Limb Fracture with the following link.
Posterior Cruciate Ligament (PCL)
Posterior cruciate ligament (PCL), one of four major ligaments of the knee, is situated at the back of the knee. It connects the thighbone (femur) to the shinbone (tibia). The PCL limits the backward movement of the shinbone. The posterior cruciate ligament is usually injured by a direct impact, such as a motor vehicle accident when the knee forcefully strikes against the dashboard or during sports participation when a twisting injury or overextension of the knee can also cause PCL injury.
Find out more about Posterior Cruciate Ligament (PCL) with the following link.
Quadriceps Active
-
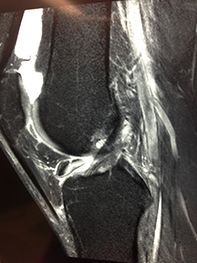
PCL Tear Hyperextension

Post Partial Menisectomy
-
Retracted Superfical MCL
Anterior Drawer
Chondrocyte Grafting
Coming soon
Find out more about Chondrocyte Grafting with the following link.
Please use the links below to get more information from the American Academy of Orthopaedic Surgeons:
Broken Bones and Injury
Common Knee Injuries
Hamstring Muscle Strain
Muscle Strains in the ThighFractures
Femur (Thighbone) Fractures in Children Growth Plate Fractures Proximal Tibia Fractures
Shinbone (Tibia) Fractures
Stress FracturesTears and Instability
Kneecap, Unstable
Meniscus, Tears of
Posterior Cruciate Ligament, Tears ofPain Syndromes
Osgood-Schlatter Disease (Knee Pain)
Runner's Knee (Patellofemoral Pain)
Shin SplintsDiseases and Syndromes
Bowed Legs
Bursitis of the Knee: Goosefoot (Pes Anserine)
Bursitis of the Knee: Kneecap (Prepatellar)
Limb Length Discrepency
Osteonecrosis of the KneeArthritis
Arthritis of the Knee
Osteoarthritis of the Knee - Frequently Asked QuestionsPain Syndromes
Burning Thigh Pain (Meralgia paresthetica)
Compartment Syndrome
Knee Pain, Adolescent Anterior
Osgood-Schlatter Disease (Knee Pain)
Runner's Knee (Patellofemoral Pain)Treatment and Rehabilitation
Osteoarthritis: Surgical Treatment
Joint Replacement
Anesthesia for Hip and Knee Replacement Surgery
Knee Replacement and Implants
Knee Replacement, Cemented and Cementless
Knee Replacement, Minimally Invasive
Knee Replacement, Osteotomy and Unicompartmental Replacement (Arthroplasty)
Total Knee ReplacementNonsurgical Treatment
Care of Casts and Splints
How to use Crutches, Canes, and Walkers
Viscosupplementation in Osteoarthritis of the KneeArthroscopy and Reconstruction
Anterior Cruciate Ligament Injury, Surgical Considerations in
Knee Arthroscopy
Meniscal TransplantsConsiderations
Postoperative Care
Knee Arthroscopy, Exercise Guide
Knee Replacement - Exercise Guide
Knee Replacement, Activities After